THESIS
Utilizing large language models for improved at-home stroke care and rehabilitation.
WEEK 1
Hello and Welcome!
This is my thesis page. Im going to use this space as an area where I explore my mental meanders, development of my tool and document the development of my prototypes.
Im so excited to take you along with me on this journey.
Let’s get straight into it, during the 2020 covid lockdown, I learnt that stroke was the 5th cause of mortality in Nepal. By 2023, it had moved up to the 3rd reason, according to the WHO.
Having parents who worked tirelessly to hold up rickety health systems in Nepal, I noticed many specialty-high resourced centers being established and creating lots of knowledge and work around thrombolyzing the blood clot that has caused the stroke, and the immediate care in the hospital that came after that. However, pain lingered, and sometimes patients would be rendered without much help for rehabilitation, especially after receiving care and returning to their hometowns in rural Nepal.
While in conversation with a neurologist, during pre thesis last semester, currently practicing in the UK, with roots in Nepal, they suggested that I should look into AI leveraging for stroke recovery and rehabilitation.
I wanted to explore ai for rehabilitation, despite understanding its effects on a population that has suffered because of Colonization.
WEEK 2
Ok, week 2 here we go. Lots of feedback after the first week and introducing our projects in class.
I spoke a little bit about my pre thesis, and how it will help lead me to my prototype. If you would like to flip thru my slides, find them here.
Anyways, our task for the week was to create our first prototype. I shared my prototype… which conveniently broke down, and I had to share a video of the working prototype instead. Classic tech stuff.
Anyways, here is a working video of my prototype.
I received a bunch of feedback from my advisors for the thesis project.
Going in I was really keen on creating an experience that honored disability and created a safe space for people with all sorts of disabilities that go beyond stroke.
After creating this prototype, my advisors suggested to focus on 1 part of the extremely long and strenuous rehabilitation journey. I wanted to focus on a simple, universal method that is used by speech therapists and physiotherapists.
WEEK 3
So, after another round of conversations with the speech therapist, I created a new prototype, focussing on 1 part of the rehabilitative journey.
I decided to stick to counting from 1 to 10, and keep the prototype super simple:
Creating that was super fun, I vibe coded that prototype and with the help of the speech therapist, and a couple other more rounds of testing and continued conversation, created the working prototype.
I was excited showing my prototype to my advisors. I took it one step further and added more refinement and research with a creative technologist, Louise Lessel. I showed her working prototype of my working prototypes, of both the physical therapy device, as well as the audio visual prototype. She taught me about shaders, and how I could create a high-tech experience for rehabilitation at a hospital, and then create a lo-fi low code version that reflects the same design elements into a phone, at-home for rural usage in Nepal. She did suggest that using AI in a low-resource context, for rural Nepalese people would be difficult to set up, both in terms of digital literacy, as well as operationalizing.
I also visited Torin Blankensmith, another creative technologist, who helped me decrease the confidence of my immersive experience, which heleped the computer read hands better, as they can come in all sorts of shapes and sizes. He told me about his work at Mt. Sinai which he created with his partner, an immersive experience.

WEEK 4
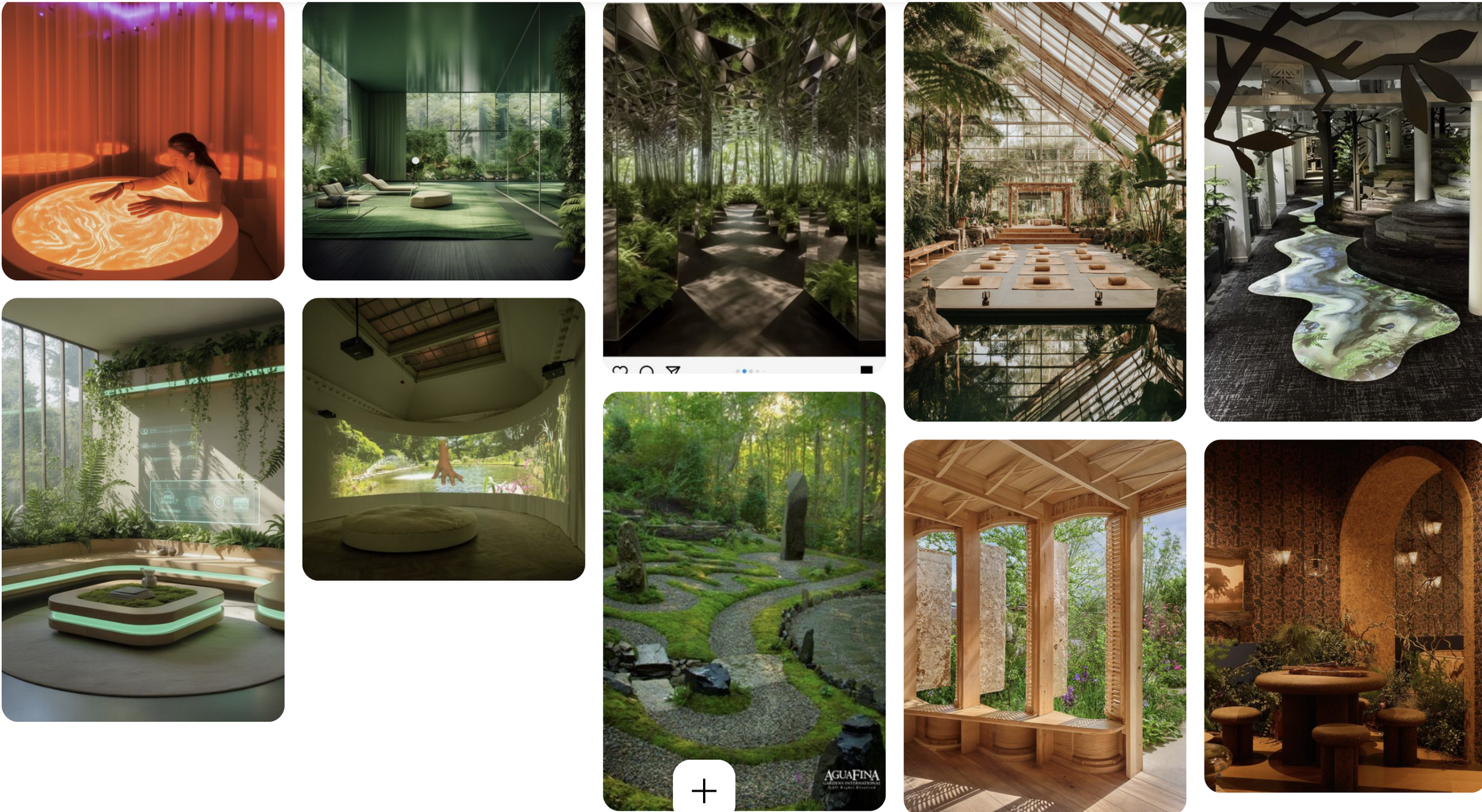
Louise Lessel also connected me to Torin’s partner, whom I will be visiting soon, Mischa who will help me demo their rehabilitative space. I will take inspiration from this experience and Ive already made a moodboard to have more clarity in what I want my experience to look and feel like:
Then I went on three gif, as advised by Louise, and found the same renders for my prototype that reflects my big hospital prototype as well.
Here is the working link of the prototype
Anyways, I reflected on the importance of grounding my AI prototype in clinical reality rather than purely speculative interaction design. I showed the concept to a speech therapist and am currently waiting to hear back. I realized that imagining how a therapist would physically sit beside a patient while interacting with the system changes everything — this is not a standalone tech product, but a co-therapy tool.
The physiotherapists provided unexpected but incredibly useful phonetic insights. They noted that words with consonants are comparatively easier than vowel-heavy words. In number articulation, 1, 2, 4, and 10 are easier. However, 3, 5, 6, 7, 8, and 9 are more difficult — with 7 and 8 being the hardest.
For vowels:
“A” and “O” are easier.
“I” and “E” are harder.
This shifted my thinking. I initially assumed vowels would be simpler, but that assumption came from a non-clinical perspective. The difficulty is not intuitive — it is embodied.
I am now thinking about how the AI should communicate this to participants. Should they know that certain sounds are neurologically harder? Would that reduce frustration? Or would it feel discouraging?
Another tension I’m grappling with is aesthetic direction. Hospital interfaces feel cold and clinical. Children’s speech apps feel gamified and overly cheerful. My audience who happen to be adult stroke survivors in Nepal, exists in neither category. The interface must feel dignified, calm, and culturally grounded, without feeling infantilizing or sterile.
This feedback is pushing me to rethink the role of AI — not as a flashy innovation, but as a quiet, adaptive companion embedded within a therapist’s care ecosystem.
Existing products in the market exist for B2B solutions, availability to clinicians, and whatever little s existing, are not very user friendly and look visually dated. Theres many tools for paediatric use, however, it is more for cognition streamlining and games, rather than for rehabilitation.
Im excited to test my prototype with patients in Nepal. The next step is to make the camera understand the mouth shapes through face recognition and ai, so the tool is able to give feedback on the shape of the mouth as well.
WEEK 5
This week was honestly a bit of a reality check.
I started exploring the idea of integrating face recognition and mouth-shape detection into the prototype. On paper, it felt like the “next obvious step.” If the system could see how your mouth moves, it could give better feedback, right?
But the more I tested and spoke to people, the more that idea started falling apart.
Technically, it’s heavy. It requires a stable camera, decent processing power, and good lighting conditions. Contextually, it also raises questions — do we really want to introduce a camera into a rehabilitation tool that is meant to feel safe and non-invasive?
And more importantly, it just didn’t feel aligned with rural Nepal.
I kept coming back to this question: who is this for?
Not for someone with the latest iPhone. Not for someone with stable WiFi. Not for someone sitting in perfect lighting conditions ready to perform for a system.
So I started pulling back.
This week was less about building and more about letting go of ideas that didn’t belong.
And weirdly, that felt like progress.
WEEK 6
This week, I leaned deeper into simplicity.
Instead of trying to expand the system, I focused on refining the existing interaction — counting from 1 to 10.
At first, it felt too small. Almost embarrassingly small for a thesis project.
But the more I sat with it, the more I realized how much depth exists in that one task.
Counting isn’t just counting.
It reveals rhythm, breath, articulation, hesitation, confidence.
And with the phonetic insights from the speech therapist, I started to see patterns:
Where users might slow down
Where they might struggle
Where encouragement matters more than correction
I began sketching out different kinds of feedback:
Not “wrong” vs “right”
But “try again slowly”
“that was close”
“take your time”
I’m starting to think the system’s tone might be more important than its intelligence.
Because in rehabilitation, how something is said matters just as much as what is said.
WEEK 7
This week I started thinking more seriously about tone and dignity.
A lot of existing speech therapy tools either feel:
overly clinical (cold, rigid, intimidating), or
overly gamified (bright, childish, almost patronizing)
And my user is neither a patient in a lab nor a child learning vowels.
They are an adult.
Someone who had a life, a voice, an identity — and is trying to regain parts of it.
So I began experimenting with:
softer visual palettes
slower transitions
less “reward-based” feedback
more presence, less noise
I also started thinking about silence.
Not everything needs a response.
Not every pause needs to be filled.
Sometimes the system should just wait.
That felt like an important shift — designing not just interaction, but space.
WEEK 8–9
SPRING BREAK 🌿
(No work. Or at least… that’s what I told myself.)
WEEK 10
Coming back from break, I looked at the project with fresh eyes — and a bit more distance.
And I realized something important:
I had been trying to make the system impressive.
But what it really needed to be was reliable.
So I reframed the project again:
Not as a high-tech AI system,
but as a low-resource, high-sensitivity tool.
This changed how I thought about everything:
Interface → must load fast
Interaction → must be obvious
Feedback → must be minimal but meaningful
Tech → must not fail easily
I also started thinking more about caregivers.
Because in Nepal, rehabilitation is not individual — it’s relational.
Families are deeply involved:
helping interpret speech
encouraging practice
sometimes speaking for the survivor
So the system isn’t just for one user.
It sits inside a small ecosystem.
And that changes the design entirely.
WEEK 11
This week, I focused more on the idea of the clinic-life gap, which is now becoming central to my thesis.
I kept thinking about something a caregiver said:
“The doctor says he’s doing well, but at home, we still don’t understand him.”
That line stayed with me.
Because it exposes the gap between:
performing well in structured environments
and communicating in real life
So I started asking:
What does “success” actually look like for this system?
Not perfect pronunciation.
Not clinical accuracy.
But maybe:
being understood by a family member
being able to ask for water
being able to participate in conversation
That shift is subtle, but it changes the goal entirely.
I’m no longer designing for performance.
I’m designing for participation.
WEEK 12
This week felt like things started coming together.
Not in a “finished” way, but in a clearer way.
I now understand that this project is not about building a perfect AI system.
It’s about designing something that:
fits within constraint
respects the user
supports existing care rather than replacing it
I also feel more confident about narrowing the scope.
Earlier, I was worried that focusing only on counting from 1–10 was too limited.
Now I see it differently.
It’s a starting point.
A controlled environment to understand:
articulation
feedback
emotional response
And from there, the system can grow.
But it has to grow carefully.
Right now, I’m focusing on:
refining the interaction
clarifying the feedback logic
keeping everything grounded in real use
This project has become quieter over time.
Less flashy.
Less ambitious in a traditional sense.
But more honest.
And I think that matters more.